This is a brachial plexus block technique with the following clinical and side effect profile :
1. Clinical profile - the whole of the upper extremity, ie. clavicle, shoulder, arm elbow, forearm, wrist, hand, fingers.
2. Side effect profile - no phrenic nerve block, no pneumothorax risk.
Background: Please refer to the following doctoral thesis -
http://specialisedpainmedicine.com.au/supraclavicular-regional-anaesthesia-revisited.html
1. Clinical profile - the whole of the upper extremity, ie. clavicle, shoulder, arm elbow, forearm, wrist, hand, fingers.
2. Side effect profile - no phrenic nerve block, no pneumothorax risk.
Background: Please refer to the following doctoral thesis -
http://specialisedpainmedicine.com.au/supraclavicular-regional-anaesthesia-revisited.html
Figure 1
Principle
If a line of tangent is passed across the anterolateral chest wall, it will run from the lateral edge of the sternocleidomastoid muscle obliquely down behind the clavicle through the supraclavicular fat pad to the brachial plexus. This tangential line can be followed with a needle under direct vision using ultrasound.
Principle
If a line of tangent is passed across the anterolateral chest wall, it will run from the lateral edge of the sternocleidomastoid muscle obliquely down behind the clavicle through the supraclavicular fat pad to the brachial plexus. This tangential line can be followed with a needle under direct vision using ultrasound.

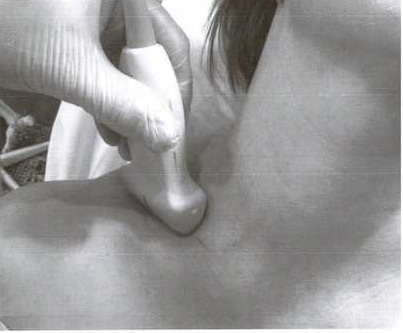
Figure 2
Practice
The ultrasound probe is placed in the supraclavicular fossa, up against the clavicle and with the medial end of the probe abutting the lateral head of the sternocleidomastoid muscle. The probe can then be adjusted to centre over the target zone as described below, as desired. The needle is introduced under the medial end of the probe.
Practice
The ultrasound probe is placed in the supraclavicular fossa, up against the clavicle and with the medial end of the probe abutting the lateral head of the sternocleidomastoid muscle. The probe can then be adjusted to centre over the target zone as described below, as desired. The needle is introduced under the medial end of the probe.
Figures 3 and 4
Sonographic Images
The images show an ovoid artery, and behind it an elongated
area of white with translucent circles within it. The elongated area is the brachial
plexus. Due to the elongated appearance of the artery and brachial plexus
resembling a comet and its tail, I nicknamed this view of the brachial plexus the
'comet tail'. The target for the block needle is within the comet tail.
Sonographic Images
The images show an ovoid artery, and behind it an elongated
area of white with translucent circles within it. The elongated area is the brachial
plexus. Due to the elongated appearance of the artery and brachial plexus
resembling a comet and its tail, I nicknamed this view of the brachial plexus the
'comet tail'. The target for the block needle is within the comet tail.


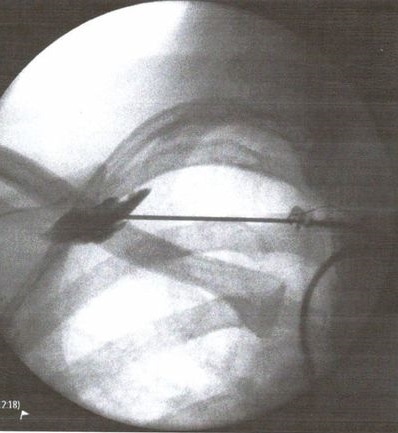
Figure 5
Scientific Foundation
The altered clinical and side effect profile related to the position of the tip of the needle, lateral to the first rib (placing it at division level) and behind the axillary artery. At this point, the surrounding bony anatomy (first rib and clavicle - part of the axillary tunnel), causes the local anaesthetic to spread to the cords laterally and the trunks medially, and the local anaesthetic spread behind the artery keeps it well away from the anteriorly placed phrenic nerve. Axillary tunnel block is neither a supraclavicular nor an infraclavicular technique; instead it sits between them. It is the only brachial plexus block supported by a doctoral thesis.
Scientific Foundation
The altered clinical and side effect profile related to the position of the tip of the needle, lateral to the first rib (placing it at division level) and behind the axillary artery. At this point, the surrounding bony anatomy (first rib and clavicle - part of the axillary tunnel), causes the local anaesthetic to spread to the cords laterally and the trunks medially, and the local anaesthetic spread behind the artery keeps it well away from the anteriorly placed phrenic nerve. Axillary tunnel block is neither a supraclavicular nor an infraclavicular technique; instead it sits between them. It is the only brachial plexus block supported by a doctoral thesis.